


Abridge On The River kwAI
There is no chance I am the first person to make that pun

Disclaimer: Newsletter and the information contained herein is not intended to be a source of advice or credit analysis with respect to the material presented, and the information and/or documents contained in this website do not constitute investment advice. Opinions contained within this letter are my own and not those of my employer.
PROCESS
Several weeks ago I attended the ViVe healthcare conference in Los Angeles. And other than being deeply upset by the fact that it was colder in LA than it was in Cincinnati in February, I had a great experience. Along with normal conference fare of meeting a lot of interesting people and learning a ton, there was one key takeaway that was deeply seared into my mind: HOSPITAL WORKERS ARE OVERWORKED.
The US Surgeon General even has a heartfelt message touching on the subject of healthcare burnout. There are medical studies tracking this issue with some pretty compelling evidence. Nearly half of health workers reported often feeling burned out in 2022, up from 32% in 2018. And while a lot of the data could easily point to a jump in this issue due to COVID, what I largely heard at ViVe is that this trend doesn’t seem to be slowing down - in fact, it’s getting worse1.
There are several considerations as to why this is happening, but one of the core reasons is burden of work. As one panelist I heard at the conference put it, a lot of this burden is driven by “paperwork” - in this sense, not literally, but time spent doing data entry, digging through case files, and updating EHRs. There was a study published last year that found the following:
The rising load of clerical tasks associated with EHRs and placed on clinicians is one of the more commonly identified reasons for burnout in medicine.39,49 Physicians have become responsible for entering not only diagnoses, orders, and visit notes but also additional administrative data of perceived low clinical value. 32 Nearly 69% of PCPs feel that most EHR clerical tasks completed by them do not require a trained physician. 13 In a survey of 282 clinicians from 3 institutions in California, Colorado, and New Mexico, of which 68% worked in primary care, the most prominent concern (86.9% of responders) about EHR use was the need for excessive data entry. 37 In fact, clinicians may need as much as 2 additional hours in electronic data entry for every hour of direct patient contact. 38 Physicians with insufficient time for documentation are 2.8 times more likely to report symptoms of burnout, 35 and in some cases clinic schedules are deliberately shortened and spots closed to allow sufficient time. 33
So it sounds like the work of updating an EHR stinks. And it’s not like our healthcare system can just eliminate EHRs or the associated clerical work. For one, like most systems of record, they are important to accurately manage processes of an organization or enterprise. But they are also heavily tied to a hospital’s ability to actually make money. Most reimbursement processes require significant EHR data in order to confirm payment for a treatment. EHR’s might be one of the best examples of regulatory capture on the planet. As a result, they are complex, important, and driving people nuts.
Enter: Abridge. The Company is an early entrant to the arena of recording patient-doctor conversations and executing clerical work on behalf of both the doctor and the patient. You can find decent demos of the product online, but the punchline is that this tool positions itself as something that greatly reduces the need for notetaking (because it is taking notes for you!) and even helps with follow ups, processes, etc.
How It Works: It is using LLMs and Natural Language Processing technology to intelligently provide a better clerical experience for doctors so that they can pay more attention to their patients and so they can do less paperwork after work. Doctors turn it on and it starts recording patient interviews and visits. Those recordings are then turned into notes, logged into an EHR, and creates follow-up tasks for the doctor such as reminders. Critically, the product is integrated with EHRs (notably EPIC, more on that later). So instead of adding a completely new portal and workflow for doctors, Abridge’s AI is allegedly baked into existing workflows. This is an important component of any AI because it actually helps with productivity, instead of just adding another thing that a person needs to figure out how to use productively. Even the greatest products have a learning curve - and as we have already established, doctor’s don’t need another piece of clerical work to keep up with.
Other Key Features:
Real Time AI Note Drafts - while a doctor is talking to a patient, the notes are taken in real time - not processed after the fact. This is pretty good compared to most NLP models out on the market. Not sure it’s defensible long term, but it’s maybe a good sign on the tech team’s capabilities.
Structured Clinical Notes - allows for the notes to be formatted in a way that is readable in the clinical setting. Provides a history of present illness, assessment & plan, and other typical sections of medical notes.
Linked Evidence - built-in auditability for trust and verification. Helps a care provider make sure that AI summaries are sourced adequately.
Multi-lingual automatic speech recognition
Integration with Epic - not really a feature, but for a healthcare company like this one, it might as well be. According to the marketing materials - clinicians will be able to harness the power of Abridge from start to finish without ever leaving Epic. A core assumption that I agree with: doctors don’t like to change their workflows. This is critical in allowing that.
It is also worth noting that for awhile, the marketing of the Company was focused largely around selling DTC - meaning directly to patients who are interacting with their doctors. They actually cite a fair amount of patients who downloaded the product (~500K as of mid-2023), but it’s hard to tell if the usage was very strong and if the Company was ever able to monetize those patients effectively. An easy explanation might be that the pivot into focused on selling into health systems is based on necessity. But maybe there is a broader network effect at play here - hard to tell.
According to a variety of interviews from the founder (where I got a bulk of my data), Abridge’s tool has been in market since Q4 2022. It’s hard to find actual user and revenue data, but it has already raised gobs of money. It has a murderer’s row of investors on the cap table: Redpoint, BVP, Lightspeed, Union Square Ventures, the list goes on. It raised a $150M Series C round in March 2024 with an assumed post-money valuation of $850M. That makes the pre-money valuation $700M. Let’s assume that this was a quick deal and that valuation number lines up closely to the ARR figure for a similar period. Assuming an 88x ARR multiple (more on that later), then the assumed ARR for Q1 2024 is in the $8M - $10M range2.
[An alternative revenue calculation would be to sum up all of the doctors in all of the systems they have listed as partners on their website (roughly 29K) and add a per-doc multiplier for an ARR calc. Let’s say it’s $250 per year per doc, that would leave them with ~$7.3M ARR. Or maybe it’s $250 per month, which would mean $87M… I had trouble nailing down per doc fee.]
Regardless of what you might think of that multiple, it’s astonishing to get to $10M in ARR in 6 quarters. When you lump that into the fact that the market is selling directly to health systems, one of the most notorious sales cycles in SaaS, it’s pretty remarkable. A key distribution advantage that they have is that they are part of Epic’s Partners & Pals program - which could theoretically open up a lot of doors for the Company. As a partner with Epic, the Company might be the first doctor notetaking tool that a health system will turn to if that health system is already an Epic customer. Why deal with the hassle of worrying about a new tool to integrate into Epic when that already comes out of the box?
PEOPLE
The founder of Abridge is Shivdev Rao, based out of Pittsburgh. He’s a practicing cardiologist at UPMC where he (his own words) “dogfoods his product and gives feedback back to his product people after doing his rounds”. He only works a couple of times a month, but it says something in-and-of-itself that he has a clinical background. On top of that, he spent the early part of his career as a Corporate Venture Capitalist for UPMC. I don’t know how UPMC sets up it’s venture group, but I have spent some time around CVCs (working with/for/near), including two hospital CVCs for which I helped to write some venture checks. Every CVC is extremely different and those differences tend to be more severe than the differences between traditional venture firms. But the one thing I can guarantee, is that Dr. Rao was thinking about NLP in the clinical room setting well before he started this Company in 2018/2019. When I started in venture in 2018, it seemed like something everyone was talking about - not an if conversation either, but a when it would happen.
I am a venture capitalist, so it’s against my own self interest to say what I am about to say: I never know how I feel about VC’s turned entrepreneurs. I have VERY STRONG opinions about the reverse (entrepreneurs turned VCs), but the other side of that two-way street sometimes vexes me. In theory, VCs are constantly surrounding themselves with innovative companies, ideas, and people. As a result, they should have a very firm grasp on what works and what doesn’t work in our innovation economy. They spend enough time telling entrepreneurs that their ideas aren’t good enough - logically, they should be very good at coming up with ideas and business models that are attractive for venture capital.
However, I have two core beliefs about VC-backed startups that rub up against this notion: (i) execution is everything and (ii) ideas are cheap. Just because the business plan sketched out on a whiteboard looks infallible, that doesn’t mean the actual business is going to succeed. On top of that, the skill set to be a VC doesn’t necessarily match the skill set to be an entrepreneur - VCs spend a lot of time thinking big thoughts, and not as much time just purely executing on ideas. I always see the following image in my head whenever I hear about VCs doing industry thesis building:

However, having operational / domain expertise is a powerful tool in company building. Especially in an industry as complex and opaque as healthcare. And so the combination of CVC + Clinical Doctor leads me to believe that Shiv is probably extremely well suited to build a company like this. When assessing teams, I do try to think through the lens of whether or not this team is in the top 1% of people trying to build this product right now. If the answer is no, it makes doing that deal a lot harder. But it’s not just about ideas and vision, they have other folks on the team as well:
Zachary Lipton (CTO and CSO) - he is both the tech guy and the science guy, which is always sorta wonky. But his chops are pretty legit. For one, he is a professor of machine learning at Carnegie Mellon, which is literally be the best Machine Learning school on the planet. He has also spent a little bit of time around startups, although it doesn’t appear that he has any hypergrowth experience.
Brian Wilson (Chief Commercial Officer) - based out of Nashville, he’s likely the guy steering the boat as far as go-to-market is concerned. He also doesn’t appear to have any hypergrowth experience, but based on his LinkedIn, he has spent a lot of time doing stuff like: enables organizations to successfully embrace their digital health strategy at the point of care. Which sounds exactly like what Abridge is trying to accomplish.
Julia Chapin (COO) - has been with the Company basically since it’s founding, and, not only that, was promoted to COO right before they closed their Series A financing in 2022. I love seeing a person climb the ranks at a startup - it’s incredibly difficult to do and shows a level of resilience that is hard to come by. She spent most of her career in the non-hypergrowth world of Google and YouTube. She also started a Company called Binti, which appears to have achieved hypergrowth after she left.
TECHNOLOGY
For most AI / Machine Learning companies (remember the term machine learning? whatever happened to that?), it’s become increasingly complicated to identify if there is anything technical about the product that is unique and defensible. With the arms race that is going on in the AI world right now, it feels like the only folks who will have defensible AI technology are either (a) extremely well funded horizontal AI tools, like OpenAI, Anthropic, etc. who nail distribution, or (b) vertical focused tools that can fine tune their models in a manner that will produce meaningfully superior results than the competition.
Abridge is definitely trying to take advantage of the second tech advantage. The colloquial3 term for this today is Data Network Effects. Part of the assumption here is likely that Abridge users will feed tons of data into the platform, which will help the platform become better. As docs and patients use the tool, the tool will learn from that usage. Some examples:
Improved recognition of medical terms better than a normal natural-language-processing tools
Improved data processing into integrated systems (aka the tool helps doctors fill out paperwork more quickly over time)
It might be able to assist with improved decisions, such as diagnoses or care pathways.
Without having used the product myself or seen a real demo (I have watched a couple of YouTube videos, but that’s about it), it’s really hard to tell if this tech advantage is possible. I will say that it does intuitively make sense - medical terminology is extremely complex and even hard to pronounce. The off-the-shelf model likely would struggle with this without some serious fine-tuning. Not only that, but medical paperwork - the processes and procedures involved in actual care for a patient - get more complicated every year. Which means building tools to help do this paperwork should be pretty tough to replicate.
The third point I made about actually helping with medical diagnoses and decision making is a larger question mark. For one, anything in that arena requires FDA approval, which is never simple. But also, who knows if any tech is really there yet - is it really good enough to provide a high confidence medical diagnosis better than a human doc and with less error? If that is hypothetically true, would the patient-doctor conversations which most decisions are based on be a great place to start building that model? Probably.
WAVE
AI is very hot in the streets right now. So much so, that there appears to be two different venture markets. One that is effectively going through a generational up cycle (AI) and another that is going through a generational down cycle (everybody else). Of course, when I say generational, I mean the generations between some very small, short-lived mammal, like a pygmy shrew or a hedgehog. From the most recent Redpoint state of the market report:
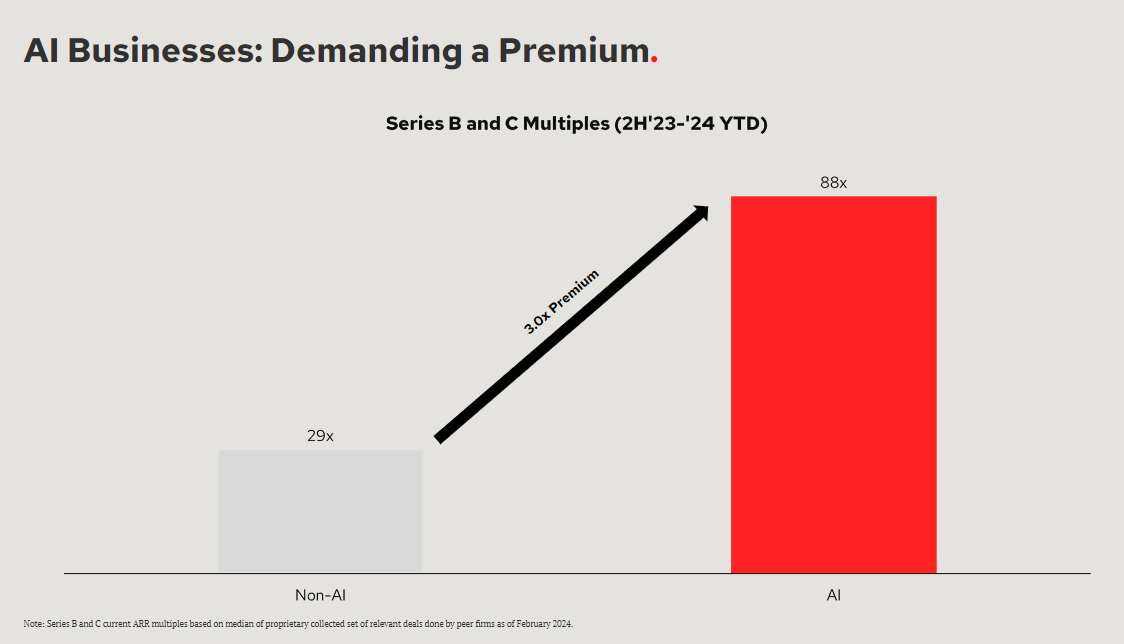
Series B and C multiples are out of this world bananas. For context, during the most recent cyclical peak of the market (2021), the Series B & C multiples were close to 105x. So even during an incredible downturn in the economic environment, some sectors are close to all time highs. And keep in mind that when people talk about multiples in the 2021 ZIRP era, the reference point is that those multiples are absolutely insane.
So what’s happening here? Simply put, the market is betting that AI is an all-time wave. Which, is a decent bet, even if you just think about it from a revenue / traction perspective. There are a lot of stories out there about pace of growth in some of these AI companies, but the most famous is probably OpenAI, who allegedly crossed a $2bn revenue run-rate in February 2024. As a reminder, ChatGPT was launched in November 2022. My daughter was born the month prior and she’s just starting to learn the words to “wheels on the bus”. Not only that, but OpenAI thinks they can double that run-rate figure by the end of 2025.
It follows that the investments into this industry are spectacular in size. Advancements in AI have been remarkable as well. The demos that seem to come out every day are something else. However, the veracity and fidelity of them leaves some questions unanswered. But one thing that seems to be an accepted truth is that the advancements of natural-language processing in the LLM space - in other words, turning speech to text and organizing this text effectively - are inevitable. If you have ever used a tool like Gong or some other notetaking app while on Zoom, you know that the speech-to-text conversion isn’t perfect, but it’s still pretty remarkable, and getting better in rapid increments. So now, the question is who is building the next iteration - the next Gong for X is now the Uber for X for the current generation.
And Gong for Doctors seems like a no-brainer. Aside from all of the detailed issues described above regarding the problems doctors face in the current environment, it’s also important to note that doctors basically spend half of their days in conversation with patients. That means that even the highest fidelity, photographic-memory-having doctor out there is going to miss some details over time. And that means that mistakes could potentially be made in the care of the patient. If there was a way to not only erase these mistakes, but maybe even make suggestions, that could be deeply appealing to all parties in the healthcare system. That’s what a Gong for Doctors is attempting to do.
It’s not just Abridge who is doing this, however. A couple of key competitors:
I am not going to go into much detail about each company, but the point is that a lot of folks are trying to ride this wave. As far as I can tell, Abridge is the one with the most amount of capital raised,4 however most of them are extremely well funded also. There is a medical note-taking AI arms race going on and a lot of the big players are getting in on the action.
Key Questions
Does the company actually have the revenue velocity that would garner this much attention? Have they been able to use their go-to-market motion and effectively penetrate the health system industry?
Does Abridge actually effectively seamlessly connect into existing workflows? If not, is this tool just making the problem worse, not better?
Do they have strong case studies showing real usage among docs that is leading to real decline in paperwork?
What are their long-term competitive differentiators in a very crowded market.
Beyond the stats and the data, I think this is one of those things that most people will be ready to believe because most people personally know someone who works in a hospital: nurses, MDs, NPs, etc. And if you know someone who works in a hospital, you likely have familiarity with the toll it can take on that person.
To be honest, I don’t feel good about this number. On the Company’s website, they only list four health systems as trusted partners. Seems like not enough, but maybe that hasn’t been updated in a while?
I say colloquially because, while there are companies out there with clear data network effects (costar, netflix, etc.), I am not sure there are a lot of true AI companies with examples of these Data Network Effects (version 2.0, if you will) that are out there today. Maybe OpenAI has some and just aren’t as well known, but I can’t think of any very obviously examples.
Not including Nuance who was acquired by Microsoft in 2022 for >$18 billion